May 12, 2015
I was talking with a surgeon at AAOS who has been using CarboJet for a while now and he made a very interesting comment about what motivated him to try the system initially. He confided that – before adopting CarboJet – he was often seeing radiolucent lines in his UKA patients’ post-ops, and some of these patients, with the normal residual post-op pain, were going to local competitive surgeons for second opinions and being told that the combination of their pain and the radiolucent lines indicated that they may have loosening and may need revision. He felt that some of his patients had been unnecessarily revised as a result of these radiolucent lines! When he substituted CarboJet for his pulsed saline lavage the radiolucencies were no longer present and a really excellent, deep cement mantle was consistently observed. This really struck me because the motivation to fix this “radiolucent line problem” was evidently strong in the mind of this surgeon, and it is quite understandable that a surgeon would be very concerned about his patients going to see another surgeon who critiques his joint replacement work and perhaps revises his patient unnecessarily. We all know that getting hospital new product approval is tough these days and that having a highly motivated surgeon to back your efforts with VACs, purchasing departments and the like, can be a key element for success. The issue described is just the kind of thing that will get a surgeon motivated!
So can we use this story to help us sell more CarboJet? We think so. We have shared this story with a couple of our sales agents and they have said they are aware of surgeons doing UKAs in their territory who are seeing some of their patients getting revised by other orthopedic practices in town. The surgeons doing the primary cases are probably unaware of some of these revisions but are surely aware of many. There are obviously a number of reasons a UKA may need an early revision, but some of our reps believe that some of their CarboJet users had the same initial motivation described above – radiolucent lines and post-op pain that is not atypical even in cases that are ultimately very successful. We think you can employ a CarboJet sales strategy in which you identify surgeons doing UKAs and then present CarboJet to them, covering all the benefits we typically highlight, but also mentioning that “a number of CarboJet users have told us that they previously saw radiolucent lines in their unis when using just pulsatile saline and felt that some of these patients were getting revised by the surgeon across town on suspicion of loosening because of these lucent lines. Once they adopted CarboJet their radiolucent lines went away and they were seeing a beautiful cement mantle no one would have concerns about”.
You might try this and see if it works for you. And experience has shown us that once a surgeon becomes familiar with CarboJet in an application like UKA (or shoulder or whatever) we wind up seeing it used on all of that surgeon’s cemented joint replacements. So this means we get our foot in the door with UKA and then get all of that surgeon’s TKA cases as well. And then of course you can work to spread usage to other surgeons in that facility too.
So let’s recap some key points to highlight when selling CarboJet to a UKA surgeon:
- UKA bone cuts are much less accessible for cleaning because of the small incision and limited operative field. It’s impossible to direct a pulsatile saline lavage jet at anything close to right angles to the bone so saline is particularly ineffective at removing fatty marrow material from the bone in UKA surgeries.
- CarboJet has a nozzle that is great at reaching back into the small incision to clean all the way back to the posterior parts of the femoral cut (40 degree angled tip nozzle).
- UKA components have limited cement-bone interface area as compared to a TKA and thus cement technique is even more critical.
- In a recent large multicenter study, aseptic loosening was the number one cause of failure of all primary knees requiring revision and accounted for 60.6% of all UKA failures!
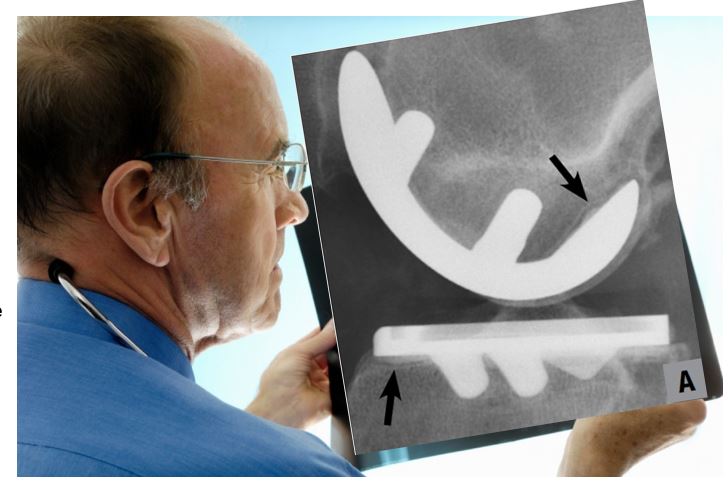
- CarboJet users are seeing markedly better cement mantles on post-op x-rays with CarboJet versus without.
- CarboJet users have told us that they previously saw radiolucent lines in their unis when using just pulsatile saline and felt that some of these patients were getting revised by the surgeon across town on suspicion of loosening because of these lucent lines. Once they adopted CarboJet their radiolucent lines went away and they were seeing a beautiful cement mantle no one would have concerns about.
- Ask for the evaluation surgery and offer a free trial! Get the surgeon to sign a request letter that you can take to purchasing to get approval for the trial.
CarboJet sales have been growing strongly for us this year and, as noted below, a remarkable 62% of CarboJet instrument sets have been sold to hospitals (versus consigned)! Leave no stone unturned and make sure you are not missing out on excellent annuity-like CarboJet business in your territory!
Best regards,
Bob Bruce
Related Materials:
- The Role of CarboJet CO2 Bone Preparation in the Reduction of Aseptic Loosening in Knee Arthroplasty
- Bone preparation in cemented partial knee replacement using pressurized CO2 gas jet system
- Dennis McGee, MD, Saint Alphonsus Medical Group, Boise, ID
- UKAs are an excellent way to get your foot in the door to new accounts. The volume is smaller than TKA (so your hospitals won’t be as concerned about the cost), and the need for CarboJet is even greater, as described in this vignette.
- Also see McGee’s CarboJet and UKA slide deck from his AAOS 2013 Booth Presentation, and these studies (with common conclusion that aseptic loosening is the number one cause of UKA failure).
- Surgeon Request Letter – CarboJet
- Have your surgeon(s) sign this and present to VAC, and/ or use these concise/ clinically supported talking points in your sales pitch.
- Mako Surgeon Marketing Opportunity (Blog Post)